An essay: Novel virus, novel inequalities, novel policies? Thoughts, impressions and insights from Florida, USA
Blog post by Elizabeth Ekren*)
Novelty defines daily life differently for people during a global pandemic. But do these novel inequalities inform novel policies? Experiences from Florida, USA reflect on how diversity in experience might drive case studies of localized policy implementation.
Emerging responses may be downplaying emerging contexts

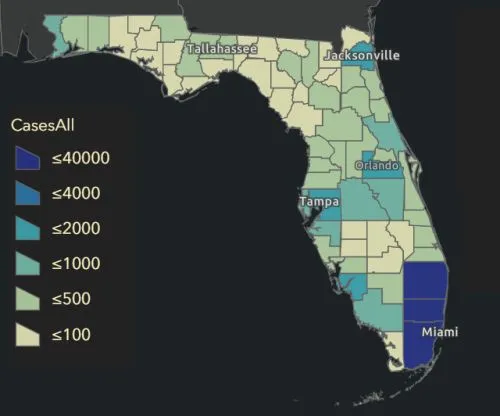
Like everywhere else in the world, coronavirus brings novelty to daily life in the United States. But novelty, apart from shared exposure to the same new pathogen, is so far looking different for many. The United States, with a population over 320 million, reports around 370 cases of coronavirus per 100,000 people. But like most everything here—where our diversity in geography, landscapes, human composition and politics manifest in every form across megacities and expansive rural farmland—the virus is proving to be more biologically prolific, and potentially socially harmful, in some places than others. New York reports nearly 2,000 cases per 100,000 residents. Montana has 52. Florida stands at 190, somewhere on the lower end, but cases are unequally dispersed within the state. Miami, the city where I live, has just over 14,000 cases, a rate of 513 per 100,000. Many rural areas in the state have less than a hundred cases total.1
The reality of the virus that its reach is anything but equal. Novel coronavirus is not only a new disease, but a new social, economic and environmental influence shaping a reality that creates unique experiences for different groups of people it affects in different ways. Ignoring contextual solutions for mitigation, management and problem solving runs the risk of neglecting the inequality of its manifestation.
Accounting for the differing manifestations of spread, Florida’s approach is trending towards being more locality driven. As I navigate my own life in Miami, a city that remains closed amidst Florida’s more targeted current reopening, I can’t help but reflect on the response with the general implementation of development policy in mind. Contextual solutions are the manner of solving most of the world’s development-related issues, be they ones of violence, politics, culture, environment or disease. But are the emerging responses to coronavirus in the United States following this trajectory and adequately considering the diversity of the disease’s emerging contexts? What points of consideration seem to be coming from Florida’s response?
Even as the initial waves of immediate emergency actions are giving way to steady-state or future-planning operations, a strong public sentiment has taken hold across the United States that there is only one way to deal with the virus across the country going forward; evasion at all costs.
Perhaps exacerbated by the heightened fear of the unknown and the well-meaning desire for the common good, the universal approach pushes for the continuation of widespread lockdowns and closures, despite the evolution of local preferences, risk considerations and disease patterns. Many leaders (including Florida’s) attempting different approaches have been chastised by others. Although individuals from different political parties seem to be obeying disease directives equally, even if their enthusiasm for doing so differs, those questioning the nature and execution of “close at all costs” narratives more vocally have been increasingly shamed in the public limelight and pejoratively associated with pillars of socially unpalatable political viewpoints.2 Instead of being treated neutrally as differences in outcomes that would make for informative case studies to analyze, the broader discussion of alternatives to “close at all costs” is becoming politicized and stigmatized.
Science aims to form generalizations from specifics, and so too should novel policy in the time of a novel virus pay close attention to the science of what works generally in controlling the spread of a new disease. At the same time, policy cannot simultaneously ignore the specific human context in which the disease occurs locally. Especially as leaders seek to implement future policies, the novel coronavirus should not warrant a novel approach that neglects critical context in addressing the local pathological and social outcomes of the disease.
Sentiments of equality can mask realities of inequality
On the one hand, unified approaches can create shared points of understanding, ways to normalize and internalize the collective experience of socioeconomic life in a diverse country being upheaved for an indefinite period of time. “We’re all in the same boat,” a common sentiment follows here, because the virus hangs in the air and lurks around all corners, waiting for us all in some way. This sentiment would tell us that the virus is a great equalizer, so we must take whatever means necessary to protect each other. Stay at home. Shut everything down. Close at all costs.
But these sentiments take away focus from a critical piece of reality: the virus is not indiscriminate. It is not uniform. As more research explores the dynamism of the virus across cases, its biological inequalities become more apparent; its potentially impaired transmission through children, increased severity with age, exacerbation through comorbidities such as diabetes or high blood pressure. Its social inequalities in the United States alone are no less concerning; higher incidence in minority and indigenous communities due to a lack of healthcare access, increasing home care burdens on women due to long-standing gender imbalances in the workplace, growing fear in the elderly and immunocompromised due to the “pre-existing conditions” of weakness that may compromise their care and make their deaths seem more justifiable to the healthy. Such immediate biological and social inequalities exist in addition to the potential longer-term consequences driving these discrepancies further, which have already begun to emerge: a 12% decrease in quarterly GDP;3 a growing 15.7% unemployment rate;4 nearly half of American small business owners forecasting the need to permanently shut down within six months;5 millions more Americans experiencing food insecurity;6 increased rates of home injuries, domestic violence, alcoholism, depression and suicide.7
Florida’s initial responses experiment with generalized and contextualized approaches
The importance of managing to local conditions seems to make sense in Florida, given that it faces its own unique considerations influencing the effects of coronavirus, just like all places. But unlike some places, the state has taken both top-down and bottom-up approaches to disease management, acting with generalized state-level interventions, but also focusing on targets of concern and allowing localities to assess conditions and determine their own actions. It is far too early to determine whether this strategy means anything significant in either direction for long-term outcomes. Even so, it positions Florida as a potential case study of what a trajectory might look like to incorporate local or targeted experiences more, albeit not exclusively, in the policymaking calculus.8
For Florida, certain factors of consideration are population spread, density and fluctuation with travel, which mean that disease may be concentrated in or affect some areas more than others. Dense, beachy cityscapes may dominate in Miami-Dade county (population 2.8 million), but the rest of Florida’s 19 million individuals are spread across urban, swampy and agricultural landscapes that span almost 1000 miles between the panhandle and southernmost keys.

Many central and northern districts are sparsely populated with suburban subdivisions or solitary rural communities. Public transportation is lacking between cities and not particularly extensive within them. At the same time, Orlando’s Disneyworld alone contributes more than 20 million tourists to the state’s annual total of 130 million, but tourism overall varies extensively by locality.9 As such, populated areas, including Miami, have been positioned to act more restrictively as needed. When popular beaches in counties north of Miami recently reopened to large crowds and high numbers of social distancing violations, local authorities immediately reinstated closures and additional restrictions. Disney theme parks closed in the middle of March—before state orders—and are not planning to reopen until July at the earliest. Given its draw of 50,000 to over 100,000 visitors a day, the targeted closure seems a relevant channel to addressing disease spread in crowds. Similarly positioned for disease clusters to take hold, cruise ships sailing out of Florida ports may remain closed until fall.
Other current and future considerations are demographic in nature, as Florida is exceptionally diverse in its composition across categories such as age, migration history and income. Different communities or subsets of people have different needs that localities or targeted interventions might be better positioned to respond to, especially as the disease progresses and secondary social consequences begin to emerge more clearly. So far, for example, the state has attempted interventions restricting the transfer of infected patients from hospitals to nursing homes, an important demographic channel to attend to given the state ranks second in the country in the number of residents older than 65.8 Immigrants, who comprise 20% of the state population and 53% of Miami’s, also stand to experience particularly difficult economic and social consequences.10 With closures acutely affecting both business owners (immigrants own over 60% of businesses in the Miami metro area) and undocumented workers, the remittances they send abroad from Miami are already on track to drop over 20%.11 For the undocumented group, who represent about 17% of Miami’s immigrant population and 20% of the state’s, the low-paying service-sector or gray market work they often take up is severely reduced or nonexistent, leaving them with little cash or recourse to attend to their immediate needs. Miami’s impoverished are positioned similarly, especially given that the city has the second-highest rate of income inequality in the nation. With just 40% of households considered middle class, and poverty disproportionally affecting black and Hispanic populations,12 these individuals are positioned to bear the already demonstrated unequal secondary burdens of disease if policy does not consider their specific circumstances effectively.13 In this regard, the response has largely relied on local governments, charities and organizations to address community needs, albeit with varying degrees of success in terms of measures such as test availability, utility bill reduction and food distribution.
Overall, Florida’s approaches have so far garnished some internal and external politicized skepticism.14 With this skepticism, many expected Florida’s (if not Miami’s) death rate to be equal to that of New York (27,000 deaths with a case-fatality ratio of 8%). But as of mid-May, Florida reports 1,800 dead, and Miami, 500 (with fatality ratios around 4.2% and 3.4% respectively). Here in Miami, once crowded beaches are still empty, although most other Florida counties began limited reopening of some businesses and restaurants on May 4. As these areas demonstrating reduced caseloads open in limited capacities, the governor has continued to empower them to maintain restrictions as they deem necessary.15
Past indications of counties shutting down in advance of state orders suggest that they will continue to manage towards the situations they face. Miami-Dade County, in response to its initial local disease spread, closed down on March 26, a week before the state’s order officially began on April 3. Local universities, schools and most businesses had begun to shutter even sooner. Cell-phone data shows self-imposed reductions in Miami foot traffic in early- to mid-March. Miami currently remains closed due to higher incidence rates and reevaluations are not happening until May 18. The city is still attempting to manage to the local conditions at hand, and case rates are generally decreasing overall, as they are at the state level. Local researchers are conducting randomized and representative anti-body testing to better inform local policy and increase understanding about the real behavior of the virus. With the positioning of the research as an “invaluable tool to help ‘manage the curve’ and get [the] community safely to work again,” its goal is to intersect science and governance with data that is not only actionable, but relevant to the local community whose policy it is meant to inform.16
Valuing diversity and learning from localities can contribute to effect policymaking
As I consider the approaches of my community and state, it seems they have not necessarily eschewed closure per se; rather, they have preferred “act as locally determined” to “close at all costs.” Are there lessons that might come from this approach? Does value exist in an approach to disease management that potentially goes against certain common sentiments?
Value exists because varied approaches lead to better understanding of costs and benefit preferences that can make policy decisions more relevant to the populations they are trying to help. As different areas in the United States have handled the dynamics of disease with different approaches, clearly none have come without cost. None have been free in terms of tradeoffs bartered, liberties curtailed, lives lost. And none, effective when judged by the cultural, political or biological conditions of their locations, could be so easily transplanted to others, where certain compromises might be valued differently, or certain situational dynamics deemed irrelevant. People have died with all approaches, but they have also survived.
Policymakers and scientists should not necessarily denounce variance in approaches. Rather, they should view it as an opportunity to analyze the contextual outcomes of success and failure systematically and collaboratively. When a given policy seems effective in one case but less so elsewhere, deeper investigation must examine the why in order to ultimately apply policies that are generalizable when relevant, but customizable when they are not. To attempt to reach a unanimous consensus on what single approach works best is misplaced because nothing will always work best in all cases with all factors considered. “We need to be careful,” our own Dr. Anthony Fauci tells us, “that we don't talk about America in totality because there are so many different levels of outbreak and of involvement with this virus throughout the country.”17 This critical point cannot be subsumed in a narrative that neglects context, diversity and inequality.
It may be unrealistic to expect more customized approaches to eliminate risk, but certainly not to balance it.18 Contextual examination may help come to a more thorough understanding of the policy nuances that might better assess disease and health, preferences and tradeoffs, openness and shut-down in local populations, especially as the virus remains with us and life together becomes the status quo.
Note: Data is current as of time of authorship. Some cited sources are updated on a continual basis.
*) The author is a junior researcher at ZEF’s Department of Political and Cultural Change
----------------------
1) Case numbers come from the Johns Hopkins University Coronavirus Resource Center.
2) https://fivethirtyeight.com/features/how-political-is-the-coronavirus-pandemic-already/
3) https://www.cbo.gov/publication/56335
4) https://www.dol.gov/ui/data.pdf
5) https://www.uschamber.com/report/special-report-coronavirus-and-small-business
6) https://hungerandhealth.feedingamerica.org/2020/03/impact-coronavirus-food-insecurity/
7) https://www.washingtonpost.com/health/2020/05/04/mental-health-coronavirus/
8) https://www.wsj.com/articles/smart-or-lucky-how-florida-dodged-the-worst-of-coronavirus-11588531865
9) https://www.visitflorida.org/media/30679/florida-visitor-economic-large-impact-study.pdf
10) Immigration statistics come from https://www.americanimmigrationcouncil.org/research/immigrants-florida and https://www.pewresearch.org/hispanic/interactives/unauthorized-immigrants-by-metro-area-table/
11) https://www.miamiherald.com/news/business/article242404271.html
12) http://carta.fiu.edu/mufi/wp-content/uploads/sites/32/2019/04/Final-Brief-Toward-a-More-Inclusive-Region.pdf
13) https://news.un.org/en/story/2020/04/1061982
14) https://www.politico.com/states/florida/story/2020/03/24/dumbest-s-desantis-takes-heat-as-he-goes-his-own-way-on-coronavirus-1268818
15) https://floridapolitics.com/archives/325112-a-round-up-of-which-florida-communities-have-stay-at-home-orders-in-place
16) https://www.miamidade.gov/releases/2020-04-24-sample-testing-results.asp
17) https://abcnews.go.com/Health/fauci-tells-david-muir-us-return-normal-light/story?id=70164631
18) https://www.theatlantic.com/ideas/archive/2020/05/quarantine-fatigue-real-and-shaming-people-wont-help/611482/